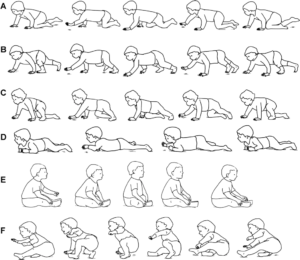
 Crawling, in general, is so important for babies to explore their environment, which is how they learn. Crawling helps them explore new things within a timely manner. But why do therapists say it is so important to crawl on hands and knees instead of the many other types of crawling, as shown in Figure 1 below? Bottom scooting, army crawling, or other types of unique crawling patterns allow infants to access their environments. However, these patterns do not provide all of the benefits that crawling on hands and knees provides.
Crawling, in general, is so important for babies to explore their environment, which is how they learn. Crawling helps them explore new things within a timely manner. But why do therapists say it is so important to crawl on hands and knees instead of the many other types of crawling, as shown in Figure 1 below? Bottom scooting, army crawling, or other types of unique crawling patterns allow infants to access their environments. However, these patterns do not provide all of the benefits that crawling on hands and knees provides.
Crawling on your hands and knees does many things to help promote development of other gross motor skills. It strengthens the shoulder girdle, helps to develop the arches of the hand, and stretches out ligaments in the wrist and hand needed for fine motor skills. These changes help support the child as they begin to do more things with their upper extremities, such as pushing to stand, climbing, and, later, handwriting skills. Crawling on hands and knees also assists with strengthening the back extensor muscle group. Strength in these muscles is crucial for standing balance and control with walking.
Alternating movements occur when crawling on hands and knees, which helps the body learn to move in a “reciprocal” pattern. Humans walk in a reciprocal way, meaning their arm swings forward as they advance the leg on the opposite side. Crawling in this way will help with the transition to walking. This type of movement also makes both sides of the brain communicate, promoting cognitive development1. Crawling on hands and knees may also help develop body scheme, motor planning, visual perception, and eye-hand coordination.
When Babies Choose Not to Crawl on Hands and Knees
Some infants may chose to bottom scoot because hands and knees crawling can be difficult. One study found that there is a link with low muscle tone, delay in gross motor skills, and hip flexion postures (knees bent up toward chest) in a group of 30 children whose mode of transportation was to bottom scoot3. The human body wants to use the least amount of energy and get the most amount of movement for it. If the child has difficulty maintaining hands and knees, they may choose a more stable posture to access their environment.
Crawling in different ways can lead to decreased hip and core strength, muscle length abnormalities, and hip range of motion restrictions in the future. This may make it difficult for children to develop complex motor skills, such as throwing, kicking, running, or jumping. While many children who never crawl have no noticeable impairments later in life, if you are noticing your child bottom scooting or crawling in a different way and are concerned, physical therapy may be able to help them gain the strength they need in order to crawl on hands and knees, giving them all benefits that crawling on hands and knees provides.
If you have questions or concerns about your child’s crawling, call MOSAIC today at (406) 388-4988 to schedule a free screen.
References:
 Your baby has a flat head. What do you do? More and more babies are getting referred to physical therapy. There are two main types of flat heads. Brachycephaly is when the back of the head is flat, causing the head to be wider than it is long. Plagiocephaly is when one side of the back of the head is flat. Brachycephaly is usually caused by a baby spending too much time lying on their back, while plagiocephaly is usually caused by a condition called torticollis.
Your baby has a flat head. What do you do? More and more babies are getting referred to physical therapy. There are two main types of flat heads. Brachycephaly is when the back of the head is flat, causing the head to be wider than it is long. Plagiocephaly is when one side of the back of the head is flat. Brachycephaly is usually caused by a baby spending too much time lying on their back, while plagiocephaly is usually caused by a condition called torticollis. What does communication at 12 months of age look like? At 12 months babies become active participants in their environments. They begin participating in familiar routines and social games adults play with them. They continue to learn language by hearing the same words/phrases paired with familiar activities, repetition of actions and words, having adults explain what is happening, reading the same books multiple times, etc. Babies also start making consistent sounds at this age and start to use these sounds or “word approximations,” with meaning and understanding. They also create babbling sounds that go on and on as if they are talking. Babies also continue to express themselves consistently using facial expressions and gestures at this age.
What does communication at 12 months of age look like? At 12 months babies become active participants in their environments. They begin participating in familiar routines and social games adults play with them. They continue to learn language by hearing the same words/phrases paired with familiar activities, repetition of actions and words, having adults explain what is happening, reading the same books multiple times, etc. Babies also start making consistent sounds at this age and start to use these sounds or “word approximations,” with meaning and understanding. They also create babbling sounds that go on and on as if they are talking. Babies also continue to express themselves consistently using facial expressions and gestures at this age.