 The most important thing when thinking about stairs is safety! Make sure you have stairs blocked off so kids can’t get to them when you aren’t watching. The next best thing is to make sure kids learn a safe and age appropriate way to go up and down stairs. Stair training starts with creeping and progresses to walking. Support and form change with increasing age, strength, and balance.
The most important thing when thinking about stairs is safety! Make sure you have stairs blocked off so kids can’t get to them when you aren’t watching. The next best thing is to make sure kids learn a safe and age appropriate way to go up and down stairs. Stair training starts with creeping and progresses to walking. Support and form change with increasing age, strength, and balance.
50% of Kids Demonstrate These Stair Milestones
- Creeps up 2 steps on hands and knees by 14 months
- Creeps backward down 3 steps without support by 16 months
- Walks up 4 steps with support, placing 1 or both feet on each step by 16 months
- Walks down 4 steps with support from only adult’s finger, placing 1 or both feet on each step by 18 months
- By 24 months, walks up 4 steps without support, placing 1 or both feet on each step
- Walks down 4 steps without support, placing 1 or both feet on each step by 25 months
- Walks up 4 steps with support, placing 1 foot on each step by 28 months
- By 36 months, walks up 4 steps without support, placing 1 foot on each step
- Walks down 4 steps without support, placing 1 foot on each step by 44 months
Ideas For Creeping Up and Down Stairs
- Have your child practice crawling over your legs to get a toy while you sit on the floor.
- Place a couch cushion on the floor and see if your child can crawl up on to it.
- Place a toy on the 2nd or 3rd step and have your child kneel at the bottom stair. Stay behind your child to protect them from falling. Assist them as needed by bringing one knee up to the next step and giving them stability to push against.
- To go down, turn your child so that his or her belly is against the stairs. Assist them coming down in this position by bringing one leg down to the lower step and then the other if they need additional help.
- Practice climbing up onto the couch and then sliding off the couch with stomach against couch cushions.
Ideas For Walking Up and Down Stairs
- Your child should be able to creep up and down stairs safely as well as walk independently.
- Stay close to your child at all times to prevent falls. When working on stairs, you should always place yourself between your child and the bottom of the stairs.
- Have your child practice walking over obstacles (such as a stick or jump rope) on the floor.
- Practice stepping up onto and down off of a short stool, curb, or other low object. Start with holding both hands and progress to 1 hand held and then to no support as your child masters each level of decreasing support. Also, alternate which foot steps up and down first.
- Place toys on the top or at the bottom of the stairs for motivation.
- Start with 2-3 steps at a time and gradually increase the number of stairs as your child’s skill improves.
- Practice carrying various items to improve balance while walking up and down stairs.
- Rehearse climbing up and down off playground equipment.
- Practice balancing on 1 leg to prepare your child for placing 1 foot on each step during stair climbing.
- Place 1 colored foot print (or a bright piece of tape) on each step as a visual cue to practice using a reciprocal pattern.
Check out Gross Motor Milestones: Single Leg Balance to learn what your child should develop next. If you have concerns regarding your child’s gross motor skills, contact MOSAIC Health & Rehab for additional suggestions or for a free screen. To learn more, check out this great milestone moments list from the CDC.
 Children’s feet come in all shapes, sizes, and positions. It is difficult to know what is typical and what is not. Additionally it’s difficult to know when to refer to a physical therapist or when to get orthotics. Common physical therapy (PT) referrals include: “toeing in”, “over pronation” and “toe walking”. Interestingly, all of these issues can be normal depending on the age of the child and their bony structure.
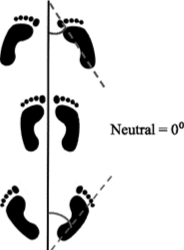
Children’s feet come in all shapes, sizes, and positions. It is difficult to know what is typical and what is not. Additionally it’s difficult to know when to refer to a physical therapist or when to get orthotics. Common physical therapy (PT) referrals include: “toeing in”, “over pronation” and “toe walking”. Interestingly, all of these issues can be normal depending on the age of the child and their bony structure.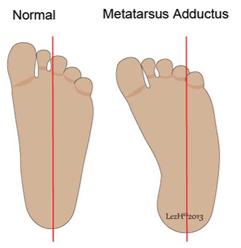 Known as the Foot Progression Angle (FPA) or “angle of gait” is between -3 and 20 degrees in most children and adults. Early walkers may show more toe-in (pigeon toed) initially. This resolves as their feet mature and become less like chubby baby feet and more defined like adult feet.
Known as the Foot Progression Angle (FPA) or “angle of gait” is between -3 and 20 degrees in most children and adults. Early walkers may show more toe-in (pigeon toed) initially. This resolves as their feet mature and become less like chubby baby feet and more defined like adult feet. This may occur when children start walking around 1 year of age. However, it should never continue past the first few weeks to months of walking. Toe walking may be due to high muscle tone in a child’s calves, sensory or vestibular issues, or from retention of primitive or infant reflexes. Physical therapy is indicated if your child continues to toe walk past the first few months of learning to walk. It rarely resolves on its own and is much easier to treat when the child is younger before habits are formed and calves/heel cords begin to tighten. Once a lack of range of motion occurs (inability to bend ankle bringing toes toward shins) there are now two issues to address: walking on toes and muscle tightness which could lead to contracture. Extreme cases will lead to bracing/ankle foot orthotics and eventually to surgery to release the Achilles tendon.
This may occur when children start walking around 1 year of age. However, it should never continue past the first few weeks to months of walking. Toe walking may be due to high muscle tone in a child’s calves, sensory or vestibular issues, or from retention of primitive or infant reflexes. Physical therapy is indicated if your child continues to toe walk past the first few months of learning to walk. It rarely resolves on its own and is much easier to treat when the child is younger before habits are formed and calves/heel cords begin to tighten. Once a lack of range of motion occurs (inability to bend ankle bringing toes toward shins) there are now two issues to address: walking on toes and muscle tightness which could lead to contracture. Extreme cases will lead to bracing/ankle foot orthotics and eventually to surgery to release the Achilles tendon.